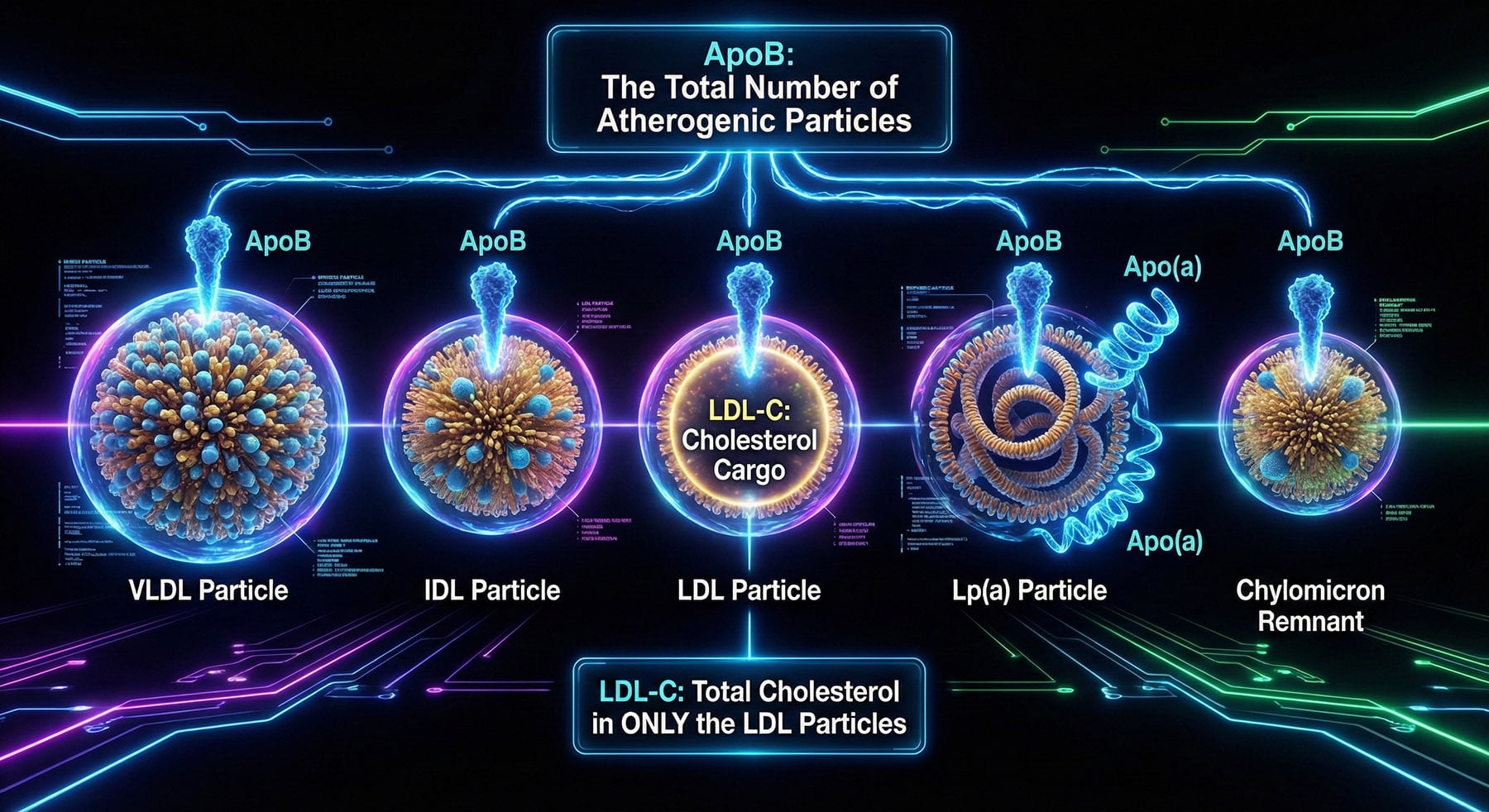
Imagine your bloodstream is a river and cholesterol is the cargo being transported. In this analogy, LDL cholesterol (LDL-C) represents the passengers, while Apolipoprotein B (ApoB) represents the boats carrying them. Standard blood tests measure the total weight of the passengers (the concentration of cholesterol). However, it is not the passengers that crash into the riverbanks (your artery walls) and cause damage; it is the boats themselves. Since every potentially dangerous lipoprotein particle—whether it is an LDL, VLDL, or IDL—contains exactly one ApoB molecule, measuring ApoB gives you a precise count of the total number of atherogenic particles in your system. This distinction is crucial because the number of particles driving into the arterial wall is the primary determinant of plaque buildup, not just how much cholesterol they carry.
This difference becomes critical when we look at “discordance,” a scenario where a patient’s LDL-C and ApoB levels do not match. You can have a “normal” amount of cholesterol passengers (low LDL-C) but distribute them across a dangerously high fleet of small, dense boats (high ApoB). This is frequently seen in people with metabolic syndrome, insulin resistance, or type 2 diabetes. In these cases, a standard lipid panel might give a false sense of security, labeling a patient as “low risk” while their high particle count actively drives atherosclerosis. Research consistently shows that when LDL-C and ApoB disagree, heart attack risk follows the ApoB number, making it the far more accurate predictor of future cardiovascular events.
Knowing your ApoB number shifts the focus from generic cholesterol lowering to precision risk management. If your LDL is normal but your ApoB is elevated, you have residual risk that lifestyle changes or medication needs to address. The 2019 European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS) guidelines now recommend ApoB measurement, particularly for patients with high triglycerides, diabetes, or obesity, where discordance is most likely. By counting the boats rather than just weighing the passengers, you and your doctor can see the true traffic on the river and take action before a crash occurs.
References
- Sniderman, A. D., et al. (2019). “Apolipoprotein B Particles and Cardiovascular Disease: A Narrative Review.” JAMA Cardiology, 4(12), 1287–1295.
- Marston, N. A., et al. (2021). “Association of Apolipoprotein B-Containing Lipoproteins and Risk of Myocardial Infarction in Individuals With and Without Atherosclerosis.” JAMA Cardiology, 7(3), 250-256.
- Mach, F., et al. (2019). “2019 ESC/EAS Guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk.” European Heart Journal, 41(1), 111–188.
Comments are closed