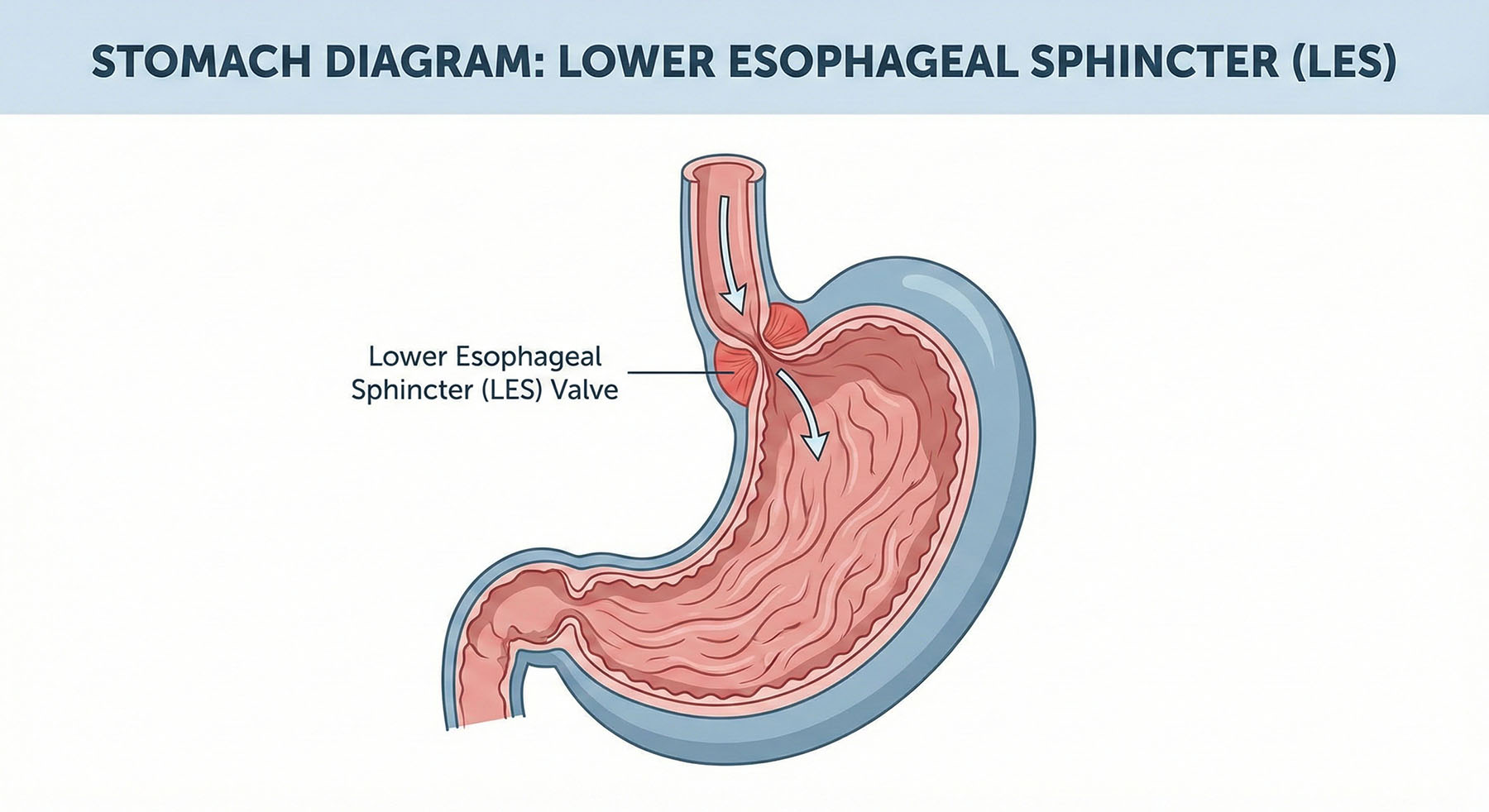
While acid reflux is commonly blamed on an excess of stomach acid, a growing body of research suggests that for many sufferers, the root cause may actually be hypochlorhydria (too little stomach acid). The logic lies in the function of the Lower Esophageal Sphincter (LES), the valve that separates the stomach from the esophagus. Adequate gastric acid is a key signaling factor for proper digestion and gastric emptying. When acid levels are insufficient—often due to aging or stress—food lingers in the stomach longer, increasing intra-abdominal pressure. This pressure can force the LES to open inappropriately, allowing even small amounts of acidic contents to splash back up, creating the burning sensation of heartburn despite the total acid volume being low [1].
A primary driver of this low-acid environment is infection by Helicobacter pylori (H. pylori). This bacterium has evolved a unique survival mechanism: it produces an enzyme called urease to neutralize stomach acid, creating a more hospitable environment for itself. Over time, an unchecked H. pylori infection can lead to atrophic gastritis, a condition where the stomach lining thins and loses the glandular cells responsible for producing acid. This not only impairs digestion but significantly increases the risk of peptic ulcers and gastric malignancies. Identifying and eradicating this bacterial infection is often the critical turning point for resolving chronic upper gastrointestinal symptoms [2].
Relying on Proton Pump Inhibitors (PPIs) to suppress symptoms without diagnosing the underlying cause can lead to significant long-term health consequences. Because stomach acid is essential for breaking down food and liberating micronutrients, chronic acid suppression is clinically linked to malabsorption of vital nutrients, including Vitamin B12, iron, magnesium, and calcium. This malabsorption can increase the risk of bone fractures and neurological issues over time. Rather than masking symptoms with lifelong medication, it is vital to undergo proper diagnostic testing—such as breath tests or stool antigen tests for H. pylori—to determine if the issue is bacterial or functional, allowing for targeted and effective treatment [3].
References
- Poynard, T., et al. (1985). “Prevalence of different types of acid reflux in patients with reflux esophagitis.” Gut, 26(11), 1196–1203. (Discusses the complexities of reflux mechanisms beyond simple hyperacidity).
- Kusters, J. G., van Vliet, A. H., & Kuipers, E. J. (2006). “Pathogenesis of Helicobacter pylori infection.” Clinical Microbiology Reviews, 19(3), 449–490. (Details how H. pylori neutralizes acid and causes atrophic gastritis).
- Heidelbaugh, J. J. (2013). “Proton pump inhibitors and risk of vitamin and mineral deficiency: evidence and clinical implications.” Therapeutic Advances in Drug Safety, 4(3), 125–133. (Evidence regarding PPI use and nutrient malabsorption).
Comments are closed